Prostate Cancer Treatment in Turkey
Prostate Cancer Treatment in Turkey is an article that aims to give you all the information you do not know about Prostate Cancer Treatment in Turkey and more. We kindly shared the main headings with you;
What is prostate cancer?
Cancer arises when the body’s cells begin to multiply out of control. Each and every cell in the body has the capacity to transform into a cancer cell and spread to different organs. Prostate cancer arises when cells in the prostate gland start to grow out of control. The prostate gland is only found in men. It generates some of the fluid that is present in semen. The prostate’s size may change as a man ages. In younger men, it is about the size of a walnut, but in older men, it can get much bigger. Continue to read to learn about prostate cancer treatment in Turkey.
What are the types of prostate cancer?
Adenocarcinomas: Makes up almost all cases of prostate cancer. The gland cells give rise to these malignancies (the cells that make the prostate fluid that is added to the semen). There are two different kinds of prostate adenocarcinoma such as acinar adenocarcinoma of the prostate and ductal adenocarcinoma of the prostate.
Small cell carcinomas: Another name for small cell prostate cancer is neuroendocrine cancer. Compared to other kinds of prostate cancer, they frequently advance more quickly. The flat cells that cover the prostate give rise to these malignancies. They typically develop and spread more quickly than prostate adenocarcinoma.
Transitional cell carcinomas: Prostate transitional cell carcinoma begins in the cells lining the tube that carries urine outside of the body (the urethra). Typically, the prostate is affected by this type of cancer after it progresses from the bladder. Rarely, though, it can begin in the prostate and migrate to the bladder opening and the tissues around it. Prostate urothelial carcinoma is another name for this. This type of prostate cancer accounts for 2 to 4 out of 100 cases (between 2 and 4%).
What are the causes of prostate cancer?
There is no direct connection between prostate cancer and any avoidable factors. Many factors determine your risk of contracting it. Risk factors for various malignancies vary. You won’t necessarily develop that cancer just because you have one or more of these risk factors. The factors that cause prostate cancer can be listed as follows,
Age: Men 75 to 79 years old are most likely to have prostate cancer.
Ethnicity: Black men are more likely than White men to develop prostate cancer.
Family history: If you have a close family who has had prostate cancer, your risk of developing the disease is increased.
Inheritance of bad genes: Some inherited defective genes can raise your risk of developing prostate cancer such as BRCA1 and BRCA2 genes and Lynch syndrome.
Weight gain and obesity: A body mass index (BMI) of 30 or more is considered obese. And a BMI of 25 to 30 is considered to be overweight. You run a higher chance of developing metastatic or advanced prostate cancer if you are overweight or obese. As a side note, prostate cancer that has spread to another area of the body is referred to as metastatic prostate cancer.
Hormones: The various organs in our body produce hormones naturally. A hormone called insulin-like growth factor 1 (IGF-1) controls healthy cell growth. According to studies, those who have high levels of IGF-1 are more likely to develop prostate cancer.
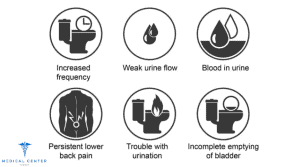
What are the symptoms of prostate cancer?
In its early stages, prostate cancer may not show any symptoms at all. More advanced prostate cancer may exhibit symptoms and signs like:
- Difficulty in urinating
- Decreased force of the urine stream
- Urine with blood in it
- A blemish in the sperm
- Bone ache
- Loss of pounds
- Erection problems
How to determine pre-cancerous condition?
Although it is not yet known for sure, some research suggests that prostate cancer initially manifests as a pre-cancerous condition. Sometimes these diseases are discovered during a man’s prostate biopsy (removal of small pieces of the prostate to look for cancer).Invest in your health, invest in a brighter future. Our comprehensive medical programs deliver real results, while you indulge in the beauty and serenity of our destination.
Prostatic intraepithelial neoplasia (PIN)
PIN causes changes in the appearance of the prostate gland cells under a microscope, but the abnormal cells don’t appear to be spreading to other regions of the prostate. Cell pattern abnormalities are categorized into the following groups:
Low-grade PIN: Prostate cell patterns seem to be practically normal.
High-grade PIN: The cell patterns appear more atypical.
It is not believed that low-grade PIN increases a man’s risk of developing prostate cancer. On the other hand, prostate cancer is hypothesized to have a potential precursor in high-grade PIN. Prostate cancer is more likely to occur in the future if high-grade PIN is discovered during a prostate biopsy. Some men get PIN in their prostates as early as their 20s. However, a lot of men never get prostate cancer even though they have PIN.
Proliferative inflammatory atrophy (PIA)
The prostate cells appear smaller than usual in PIA, and the area exhibits symptoms of inflammation. Although PIA is not cancer, experts think it can occasionally cause high-grade PIN or perhaps prostate cancer.
What is the importance of early diagnosis for prostate cancer?
Prostate cancer can be treated successfully and with less severe side effects if caught early. When discovered too late, it can, however, have a number of detrimental repercussions on the patients’ and their families’ life. Reducing the number of men diagnosed with incurable advanced prostate cancer would be one of the easiest ways to ease the pressures on individuals, their families, and the health centers. For both patients and the health services, successful early identification of prostate cancer is beneficial.
What are the side effects of prostate cancer treatment?
Advanced prostate cancer is defined as having spread outside the prostate gland. At this stage, your cancer is more likely to lead to complications like pain, erection issues, and incontinence. The medications, surgery or radiation you might receive to treat your cancer could have adverse effects in addition to the illness itself. Many of the potential issues or side effects can be managed with the right actions. Some possible side effects are listed below.
Tiredness: You may have fatigue as a result of prostate cancer or its treatments, including radiation, chemotherapy, and hormone therapy. Low red blood cell counts that can impact your energy levels are another side effect of treatment.
Erectile dysfunction: It may be challenging to achieve or maintain an erection due to prostate cancer, its therapies, or even the stress of coping with cancer. Erectile dysfunction is the term for this condition (ED). The nerves that surround your prostate and assist regulate erections can be harmed by cancer. The nerves in the area or the blood flow to the area can potentially be harmed by surgery, radiation, or hormone therapy.
Difficulties with bladder control: You may struggle to maintain bladder control after surgery for prostate cancer or other therapies. Your ability to regulate your urination may be impaired or you may leak urine due to nerve and muscle damage.
Pain: Pain from advanced prostate cancer can take many different forms. You might experience bone pain, which frequently feels like a dull aching if it extends to your bones. Your tumor might impinge on a nerve, which might result in a burning or stabbing sensation. If you’re in agony, talk to your doctor.
What is the importance of choosing the right treatment?
To help you choose the course of treatment that best suits your needs, it’s crucial to review all of your available alternatives with your doctors, including their aims and any potential adverse effects. Some crucial considerations include,
- Your cancer’s grade and stage
- Age and anticipated lifespan
- Any more severe medical conditions you have
- Your thoughts (as well as your doctor’s) in relation to the requirement for immediate cancer treatment
- The possibility that your cancer will be cured by treatment
- Your thoughts regarding the potential adverse effects of each treatment
What is prostate cancer treatment in Turkey?
You may ask yourself “What is the prostate cancer treatment in Turkey?”. Here are some of the treatment types that we have given detailed information for you,
Surgery
If it is believed that prostate cancer has not spread outside of the gland, surgery is frequently used to try to cure it. A radical prostatectomy is the most common procedure used to treat prostate cancer. The surgeon performs this procedure to completely remove the prostate gland as well as some of the tissue surrounding it, including the seminal vesicles.
Radical retropubic prostatectomy
The surgeon makes an incision (cut) in your lower abdomen from the belly button to the pubic bone in order to perform this open procedure. During the procedure, you will either be given sedation and general anesthesia (falling asleep) or spinal or epidural anesthesia (numbing the lower half of the body). The surgeon may also remove some of these lymph nodes at this time if there is a chance that cancer has spread to nearby lymph nodes (based on your PSA level, the results of your prostate biopsy, and other factors). The nodes are delivered to the lab to be examined for the presence of cancer cells. The surgeon might decide not to proceed with the surgery if cancer cells are discovered in any of the nodes. This is because it’s unlikely that surgery will be able to cure cancer, and removing the prostate could have negative consequences. After the prostate is removed, a catheter (a small, flexible tube) will be inserted in your penis to assist with bladder drainage while you are still unconscious. While you heal, the catheter will often remain in place for 1 to 2 weeks. After the catheter is taken out, you can urinate on your own. After the surgery, you’ll likely spend a few days in the hospital, and your activities will be restricted for a few weeks.
Radical Perineal prostatectomy
The cut (incision) in this open procedure is made by the surgeon in the skin between the anus and scrotum (the perineum). This method is less frequently employed since it increases the risk of erection issues and because it is impossible to remove the adjacent lymph nodes. However, if you don’t need lymph nodes removed and aren’t concerned about erections, it is frequently a faster procedure and may be an alternative. Additionally, it might be applied if you have additional medical issues that make retropubic surgery challenging for you. If done correctly, it can be just as therapeutic as the retropubic approach. The retropubic prostatectomy may cause more pain, while the perineal procedure may have a quicker recovery.
Laparoscopic radical prostatectomy
In order to remove the prostate during a laparoscopic radical prostatectomy (LRP), the surgeon inserts special long instruments through a series of tiny abdominal wall incisions. The surgeon can view the body thanks to one of the devices’ little video cameras on the end. In comparison to open radical prostatectomy, laparoscopic prostatectomy has some benefits, including less blood loss and pain, shorter hospital stays (typically no longer than a day), quicker recovery times, and a shorter time the catheter needs to stay in the bladder. Major side effects from LRP, such as erection issues and incontinence, appear to occur at roughly the same rates as with open prostatectomies. With this method, bladder control recovery might be slightly delayed. The success of either procedure appears to be primarily influenced by the experience and skill of the surgeon, even though more long-term studies are required to compare the side effects and likelihood of recurrence between open prostatectomy and LRP.
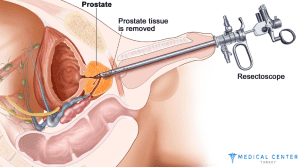
Transurethral resection of the prostate (TURP)
During this operation, the surgeon removes the inner part of the prostate gland that surrounds the urethra (the tube through which urine leaves the bladder). The skin is not cut with this surgery. An instrument called a resectoscope is passed through the tip of the penis into the urethra to the level of the prostate. Once it is in place, either electricity is passed through a wire to heat it or a laser is used to cut or vaporize the tissue. Spinal anesthesia (which numbs the lower half of your body) or general anesthesia (where you are asleep) is used.
What are the risks of prostate cancer surgery?
Issues that may arise during or right after the procedure include:
- Effects of anesthesia
- Bleeding after the procedure
- A blood clot in the lung or in the legs organs nearby are harmed
- A surgical site infection
Radiotherapy
The main types of radiation therapy used for prostate cancer are:
External beam radiation
In EBRT, a machine outside the body directs radiation beams at the prostate gland. If cancer has progressed to a specific area of bone, this form of radiation can be used to relieve symptoms like bone pain or to try to treat earlier stages of the disease. Depending on the reason for the radiation, you will often visit an outpatient facility for treatment five days a week for at least a few weeks. Every procedure is very similar to having an x-ray. While there is more radiation used than in an x-ray, the treatment is usually painless. Even though the setup process, which involves getting you ready for treatment, takes longer, each treatment only lasts a few minutes. There are several techniques such as Three-dimensional conformal radiation therapy (3D-CRT), Intensity-modulated radiation therapy (IMRT), Stereotactic body radiation therapy (SBRT), and Proton beam radiation therapy to apply this treatment.
Brachytherapy
Small radioactive pellets or “seeds,” each about the size of a grain of rice, are used during brachytherapy, also known as seed implantation or interstitial radiation therapy. You put these pellets right into your prostate. Only males with early-stage, somewhat slow-growing prostate cancer typically receive brachytherapy alone (low-grade). Men who have a higher chance of cancer spreading outside the prostate may choose brachytherapy in combination with external radiation. Other issues also restrict the use of brachytherapy. The risk of urinary side effects may be increased in men who have had a transurethral resection of the prostate (TURP) or in those who already have urinary issues. Men with large prostate glands may find that brachytherapy is less effective since it may be difficult to implant the seeds in all of the necessary areas. Getting a few months of hormone therapy beforehand to reduce the prostate may be one method to get around this.
Radiopharmaceuticals
Drugs with radioactive components are referred to as radiopharmaceuticals. To reach cancer cells that have spread to other body areas, they are injected into a vein and move through the circulation. The radiation these medications release later destroys the cancer cells. (The radiation they employ goes a very short distance, limiting adverse effects.) These medications can reach cancer everywhere in the body, unlike other forms of radiation.
Radiopharmaceuticals that target PSMA
On prostate cancer cells, the protein known as PSMA is frequently present in high concentrations. The radiopharmaceutical lutetium Lu 177 vipivotide tetraxetan, also known as 177Lu-PSMA-617 or Pluvicto, attaches to PSMA and delivers radiation to prostate cancer cells directly.
Prostate cancer that has spread and has already had hormone therapy and chemotherapy can be treated with this medication. The PSMA protein must also be present in the cancer cells. Before prescribing this medication, your doctor will order a PSMA PET scan to make sure the cancer cells contain PSMA. The usual administration schedule for this medication is once every six weeks for up to six doses, administered intravenously (IV).
Radiopharmaceuticals that target bones
In order to treat prostate cancer that has gone to the bones, several radiopharmaceuticals are made to settle there. To treat prostate cancer that has migrated to the bones, radiopharmaceuticals include: Strontium-89 (Metastron), Samarium-153 (Quadramet), Radium-223 (Xofigo).
Cryotherapy
Using extremely low temperatures to freeze and kill prostate cancer cells as well as the majority of the prostate is known as cryotherapy (also known as cryosurgery or cryoablation). Although it is occasionally referred to as cryosurgery, it is not a form of surgery.
When it is used?
After radiation therapy, cryotherapy may be performed if cancer has returned. It might be a possibility for men with early-stage, low-risk prostate cancer who are unable to undergo surgery or radiation treatment. Cryotherapy is not typically the first course of treatment for prostate cancer, though.
How it is performed?
The lower half of your body must be sedated for this type of treatment, either with spinal or epidural anesthesia or under general anesthesia (you are asleep). The physician inserts a number of hollow probes (needles) through the skin between the anus and scrotum and into the prostate using transrectal ultrasound (TRUS). The prostate is then frozen and destroyed by passing extremely cold gases through the needles. The doctor carefully monitors the ultrasonography throughout the treatment to make sure the prostate is destroyed without causing too much harm to neighboring tissues. During the procedure, a catheter is inserted through the urethra with warm salt water to prevent it from freezing. In order to allow the bladder to drain while you heal, the catheter is kept in place for a few weeks after the procedure. You might need to spend the night in the hospital after the procedure, although many men return home the same day. Given that cryotherapy is less invasive than surgery, there is typically less blood loss, less time spent in the hospital, a quicker recovery, and less pain. However, medical professionals know substantially less about cryotherapy’s long-term efficacy than they do about surgery or radiation therapy.
Chemotherapy
Anti-cancer medications are administered orally or through venous injections during chemotherapy (chemo). Most cancer cells in the body are reached by these medications through the bloodstream.
When is chemotherapy used?
When hormone therapy fails to treat prostate cancer that has spread outside the prostate gland, chemotherapy may be employed. Recent studies have also suggested that chemotherapy combined with hormone therapy may be beneficial. However, chemotherapy is not a typical treatment for early-stage prostate cancer.
Chemo drugs used to treat prostate cancer
Chemotherapy medicines are normally administered one at a time for prostate cancer. Among the chemotherapy medications used to treat prostate cancer are:
- Docetaxel (Taxotere)
- Cabazitaxel (Jevtana)
- Estramustine with Mitoxantrone (Novantrone) (Emcyt)

How it is administered?
Prostate cancer chemotherapy is often administered intravenously (IV), either as an infusion over a predetermined period of time. This can be carried out in a hospital setting, a chemotherapy clinic, or a doctor’s office. Some medications are administered as pills, such as estramustine.
Immunotherapy
Immunotherapy is the use of drugs to help the body’s immune system recognize and more efficiently eliminate cancer cells. Prostate cancer can be treated with certain immunotherapies such as the cancer vaccination called Sipuleucel-T (Provenge).
Hormone Therapy
When it is used?
Uses for hormone treatment include,
- If your cancer has progressed too far for surgery or radiation to be effective, or if you are unable to receive these treatments for any reason
- If cancer is still present or returns after receiving surgery or radiation therapy
- If you are at a higher risk of cancer returning after treatment (based on a high Gleason score, high PSA level, and/or growth of cancer outside the prostate)
- While trying to reduce cancer before radiation to increase the effectiveness of the treatment.
What are the hormone therapy types?
Treatment to lower testicular androgen levels
ADT, also known as androgen deprivation therapy, reduces the number of androgens produced by the testicles through surgery or medication.
Treatment to lower androgen levels from other parts of the body
LHRH agonists and antagonists can inhibit the production of androgens in the testicles, but cells in other regions of the body, including the adrenal glands and prostate cancer cells, can continue to produce male hormones that can promote the growth of cancer. Some medications such as Abiraterone and Ketoconazole can stop these cells from producing androgens.
You can easily request a personalized treatment plan and receive your free quote by clicking the image below.
![]()
For more detailed information and to inquire about anything you are curious about, feel free to contact us anytime. Click the link below to get in touch with our team.